




That HIV does not cause AIDS is again demonstrated, this time in a doctoral thesis, “Endogenous retroviruses as confounding factors in the pathogenesis of AIDS”, by Chiara Matteuzzi, mentored by Dr. Stefania Pacini and Dr. Marco Ruggiero. The work has just been accepted (with maximum marks) at the University of Florence, is in English, and is publicly available. The presentation was in Italian.
The literature review mentions Montagnier’s longstanding view that sound immune systems withstand HIV, unpublished work of Dr. Christl Meyer suggesting that HIV is an evolutionary adapted and partly active variable and heritable gene construct of our immune (MHC/HLA)-system, De Harven’s discussion of human endogenous retroviruses as confounding factors in AIDS pathogenesis, and Yamamoto’s demonstration that stimulation of the immune system can eradicate HIV.
The experimental part of the thesis built on Yamamoto’s work, as described in the Abstract:
“Results
We demonstrated that GcMAF stimulated human monocyte proliferation and survival and that this response was associated with VDR gene polymorphisms. Since these results were obtained in peripheral blood mononuclear cells, an interplay between lymphocytes expressing VDR and GcMAF- stimulated monocytes producing vitamin D has to be assumed. The effect was dose-dependent and maximal stimulation was achieved using 100 pg/ml. GcMAF sustained cell viability for about 98 h whereas un- stimulated cells were no longer viable after 48 h, as if GcMAF had rescued monocytes from apoptosis. Heparin inhibited the stimulatory effect of GcMAF by binding the N-acetylgalactosamine moiety of GcMAF. GcMAF stimulated cAMP formation in a dose-dependent manner. GcMAF inihibited PGE 2 – and MCF-7 (human breast cancer cell)-stimulated angiogenesis in chick embryo chorionallantoic membrane (CAM) assay. Discussion
GcAMF-induced increase of cAMP formation could account for its anti-angiogenetic effect since it was demonstrated that elevated cAMP level inhibited angiogenesis in CAM assay (J Vasc Res 31:195-204, 1994). GcMAF-induced inhibition of angiogenesis could then be crucial in determining its therapeutic effects in conditions where angiogenesis plays a key role in the progression of the disease, from cancer (Exp Cell Res 316:1304-8, 2010) to HIV infection (Angiogenesis 5: 141–151, 2002). In addition, the CAM assay proved to be a rapid, simple and inexpensive method to determine the relative potencies of different GcMAF preparations and their stability; for example, we observed that storage at room temperature for 15 days decreased GcMAF potency by about 50%. These data could prove useful for upcoming clinical trials on GcMAF. In fact, GcMAF is being sold over the internet and it appears that several people are already assuming GcMAF to treat diseases as diverse as cancer and HIV infection.”
Posts Tagged ‘Etienne de Harven’
Further HIV/AIDS Enlightenment out of Italy
Posted by Henry Bauer on 2010/10/21
Posted in HIV does not cause AIDS, HIV skepticism | Tagged: Chiara Matteuzzi, Christl Meyer, Etienne de Harven, Marco Ruggiero, Nobuto Yamamoto, Stefania Pacini | 5 Comments »
The Social Psychology of “Denialist” Scientists — Kalichman’s Komical Kaper #2, part 2
Posted by Henry Bauer on 2009/03/18
Scientists, we are instructed by Kalichman, are “by their nature and training systematic and objective” (p. 112; see “Kalichman’s Komical Kaper #2: The Social Psychology of Scientists”, 14 March 2009). That raises a seemingly obvious question:
How or why did some “systematic and objective” scientists become “AIDS denialists”?
I find no explanation for this in Kalichman’s book, even though he places quite a few of us in that category. For example, there’s Kelly Brennan-Jones, like Kalichman a psychologist and therefore also a scientist, and one for whom Kalichman had much respect and from whom he had solicited a book review: “I knew her work dating back to my years in graduate school. I knew Kelly Brennan-Jones was trained at a superlative university by some of the best social psychologists in the country” (p. xiii).
But, it turns out, Brennan-Jones differs with Kalichman about HIV/AIDS.
“My reaction was one of absolute outrage. I mean I was really angry. I was in an emotional upheaval. I surprised everyone around me, including myself, by my seemingly irrational reaction. How could someone I knew to be intelligent, well-trained as a scientist at a respectable university and in a position of influence over college students endorse a book that everyone surely knows is outdated, biased, and of little more value than that worthy of a doorstop?” (p. xiii).
Thus Kalichman describes how he himself lapsed from systemic objectivity and became irrational (though only “seemingly” so, whatever that means), but he doesn’t give a convincing explanation for why it happened. Surely that a fellow psychologist differs with him over a scientific issue can’t be the explanation — if it were, then psychologists would be in a continual state of irrational anger and outrage, given that there are disagreements over so many quite fundamental issues in psychology and psychotherapy. Nor does Kalichman suggest what might have pushed the respected Brennan-Jones, senior to Kalichman though perhaps no more distinguished, out of her customary systematic objectivity — if indeed that’s the case; Kalichman nowhere establishes that there’s anything non-objective about doubting HIV/AIDS theory, he just takes it for granted. He doesn’t even enlighten us about what convinced him personally of that. But consider the matter from Kalichman’s viewpoint for the moment; doesn’t that immediately raise the question, why did Brennan-Jones, an outstanding, systematic, objective scientist for many years, lose those attributes?
The same conundrum applies to others whom Kalichman takes to task as “denialists”. There’s Peter Duesberg, pioneer acclaimed retrovirologist, who isolated the first oncogene in 1970 and was elected to the National Academy in 1986 (p. 175) — yet who almost immediately thereafter lost the scientific attributes he had exemplified during a quarter century of highly distinguished research.
Then there’s David Rasnick (pp. 176-77), competent enough to have worked on proteases (albeit only in rats), who also apparently lost his scientific marbles in middle age or later.
Dr. Matthias Rath is not included among “denialist” scientists in Kalichman’s Appendix B, but he is referred to throughout the book as a German vitamin entrepreneur and “AIDS denialist”. It fails to be mentioned that Rath had worked closely with one of the 20th century’s leading scientists, Linus Pauling. Apparently Rath, a PhD scientist, also somehow lost his systematic objectivity in middle age or thereabouts.
Harvey Bialy had been systematically objective enough to garner a PhD in molecular biology from Berkeley. Kalichman (p. 177) appears to think he wasn’t that great a scientist, though, since he published only 27 articles and was merely an editor for a while at one the leading medical-scientific journals. At any rate, at some stage Bialy, too, apparently lost any remaining systematic objectivity and lapsed into denialism.
Then there’s the sad case of Kary Mullis (pp. 177-8), a Nobel Laureate who happens to be also an “AIDS denialist”, having evidently lost his Nobel-quality systematic objectivity at some time or other. One of the things responsible for that fall from grace, no doubt, was that Mullis persistently asked everyone he encountered to please give him citations to the specific publications that prove HIV to be the cause of AIDS; and he never received a responsive answer. Perhaps that’s enough to drive anyone out of systematic objectivity.
And so it continues. Charles Geshekter (pp. 178-9) had been a systematic, objective social scientist (historian) until he contracted denialism. Claus Koehnlein (p. 179) too — though he had been only a practicing physician, not a researcher, not a scientist, so perhaps he never had been systematically objective. The Perth Group (pp. 179-80) has several doctors and scientists who were infected with denialism around mid-career. There’s also Etienne de Harven (p. 180), formerly of the University of Toronto and the Sloan-Kettering Institute. Roberto Giraldo, who might never have been very systematically objective because his medical degree was only from South America and he had been merely a medical technologist in New York (p. 181). Mohammed Al-Bayati (p. 181), PhD from the University of California at Davis, somehow became unsystematic and unobjective at some time thereafter. Lynn Margulis (pp. 181-2), who was elected to the National Academy in 1983, is rightly famous for having discovered the mechanism of symbiosis by which evolution advances in leaps rather than by infinitesimally slow natural selection from genetic mutations; however, she too suffered a breakdown of systematic objectivity as the years went by.
And then (p. 182) there are a couple of mathematicians, Serge Lang and Rebecca Culshaw. Of course, the majority view is that mathematics isn’t a science, neither “hard” nor soft, and so maybe mathematicians lack systematic objectivity to begin with. On the other hand, it’s also a majority view that mathematics is the most rigorously logical enterprise of all — all of pure mathematics is the following of axioms to their logical conclusions.
We know, too, that the denialist scientists named in Kalichman’s book are the merest tip of a proverbial iceberg, because there are hundreds more PhDs and MDs among AIDS Rethinkers.
And yet, despite having all these examples to work with, Kalichman offers no explanation for how or why scientists morph from systematic objectivity into wacky denialism.
To fill this vacuum (vacuity?) left by Kalichman, I’ll venture a suggestion.
The clue, I think — as with HIV/AIDS itself — is the matter of age. One of the curiosities of “HIV” is that it “infects” chiefly individuals who are in the prime of adult life, 35-45 years. (And, curiously enough, as I’ve remarked in several blog posts, after a “latent period” of healthy life averaging 10 years, followed by many years of “living with HIV/AIDS” while being kept alive by antiretroviral drugs, they still die chiefly at ages 35-45).
We have a rather similarly curious situation with “AIDS denialism”: It strikes people at relatively advanced ages and typically after decades of healthy systematic objectivity.
However, if one looks more carefully into the histories of these sufferers from denialism, one can often detect some early warning signs of a tendency to deviate from the systematic objectivity of their colleagues and to strike out in new directions, to have different ideas, to be creative and innovative; but this only becomes extreme decades later, when it blossoms into full-blown AIDS denialism.
Evidently, AIDS denialism in scientists, like AIDS in people at large, is brought on by a very slow-working infection that becomes manifest and serious only a decade or more later. Obviously the cause of denialism is, as with AIDS, a lentivirus.
“HIV”, of course, is the type specimen of the species “pathogenic lentivirus”, since the earlier and very first lentivirus, which causes kuru, turned out to be a prion and not a virus at all. We know that one mode of transmission of “HIV” is from mother to child. We further know that there is a genetic predisposition to contract “HIV”, in particular, African genes predispose to contracting “HIV”.
By analogy, we can expect that the “denialist” lentivirus is also sometimes passed on from mother to child, or at least “within families” like HTLV-I and II (p. 114 in Gallo, Virus Hunting, 1991) — there is a correlation between the intellectual qualities of parents and children, after all. And there’s also a genetic predisposition to AIDS denialism: Germanic genes predispose to denialism, according to Kalichman (pp. 54, 145; there’ll be more about this in “The German Connection —Kalichman’s not-so-Komical Kaper #3”).
Kalichman has identified other characteristics of denialists as well. Most notably, they are suspicious people and conspiracy theorists (e.g., p. 13 ff. & chapter 4). But this raises the same problem as denialism itself: Why did so many now-denialist scientists contract these conditions only after decades of unexceptionable, even distinguished research?
Obviously, again, it’s that lentivirus. As “HIV” is capable of explaining every form of deviance from physical health, so the denialist lentivirus is capable of explaining every form of deviance from mental health.
AIDS scientists and AIDStruthers have had no success in protecting against the denialist lentivirus through education. Indeed, as the prominent AIDS scientists praising Kalichman’s work have testified, denialism has become a major threat to public health. Since we know that there’s a genetic predisposition to it, perhaps it will turn out that gene therapy (disabling or modifying Germanic genes) is the only really effective means of prevention — just as with HIV, where abstinence, condoms, microbicides, and vaccines have all failed miserably (“HIV gene therapy trial promising”).
Posted in experts, HIV and race, HIV in children, HIV transmission, HIV varies with age, vaccines | Tagged: AIDS denialism and gene therapy, “AIDS denialists” as often German, Charles Geshekter, David Rasnick, denialist lentivirus, Etienne de Harven, Harvey Bialy, HTLV, Kalichman’s Komical Kaper, Kary Mullis, Kelly Brennan-Jones, Lynn Margulis, Matthias Rath, Mohammed Al-Bayati, Perth Group, Peter Duesberg, Rebecca Culshaw, Roberto Giraldo, Serge Lang | 19 Comments »
NATURE leads — in censorship and illogic
Posted by Henry Bauer on 2008/12/15
NATURE honored World AIDS Day with an editorial, “The cost of silence?” [4 December, 456: 545], that’s classically AIDStruthian. It cites the Chigwere et al. claim of lives lost in South Africa as a result of failure to provide antiretroviral drugs [for deconstruction of that claim, see “Poison in South Africa”, 26 October 2008]. The AIDStruthiness of the piece is underscored by its citation of a Nattrass article that managed to reach the same conclusion as Chigwerde et al.
NATURE’s illogic is stunningly exemplified by the editorial’s concluding paragraph:
“In retrospect, the [Mbeki advisory] panel, constituted as it was, should never have been supported. Yet several of the country’s key scientific institutions explicitly endorsed its establishment, and also desisted from criticizing Mbeki. Along with his cabinet, they bear some culpability for the consequences that have now been documented. There is a moral to this tragic tale that may prove relevant in other contexts. In a young democracy with a historically hierarchical culture, and with attitudes often hardened by a colonial past, scientific institutions need not only to guard their independence fiercely but also to make their reasoned voices heard above the fray of political sycophancy” [emphasis added].
The editorial writer evidently thinks that scientific institutions are fiercely guarding their independence only when they take a stand congenial to the editorial writer, in other words, when they parrot the mainstream consensus. I prescribe a short course in history of science, with special emphasis on the role of unorthodox views in the progress of science [start perhaps with references 24, 25, 35 in “Science Studies 101: Why is HIV/AIDS ‘science’ so unreliable?”, 18 July 2008]. As history of science knows, the mainstream consensus always opposes the most striking progress.
(Note too that “young democracy with a historically hierarchical culture” is not only condescending, it implies that there’s no need, in OUR aged democracies which have no hierarchical structure, to worry about political sycophancy. Course work in social and political science as well as in science studies is evidently needed quite badly by NATURE’s editorial staff.)
NATURE’s exclusion of claims that promise striking progress was summed up nicely by Nobelist Paul Lauterbur: “You could write the entire history of science in the last 50 years in terms of papers rejected by Science or Nature” [cited by Michael Goodspeed, “Science and the Coming Dark Age”, rense.com, accessed 10 October 2004].
Gordon Stewart has experienced NATURE’s censorship perhaps as much as anyone (see “A paradigm under pressure: HIV-AIDS model owes popularity to wide-spread censorship”, Index on Censorship (UK) 3; http://www.virusmyth. net/aids/data/gsparadigm.htm), yet he has continued to offer the magazine the opportunity to live up to scientific ideals of open discussion. Most recently, he sent a calm and measured response to the “Cost of silence” editorial, and was rewarded by an instant rejection by return of e-mail:
“Dear Dr Stewart
Thank you for your Correspondence submission, which we regret we are unable to publish. Pressure on our limited space is severe, so we can offer to publish only a very few of the many submissions we receive.
Naturally, I am sorry to convey a negative response in this instance.
Thank you again for writing to us.
Yours sincerely
Jayne Henderson, Correspondence, Nature”.
Stewart then enlisted Christian Fiala, Etienne de Harven and me and re-submitted under our joint signatures. The rejection came again by instant return e-mail, though this time signed (though not necessarily in person, of course) by the chief executive editorial honcho:
“Dear Dr Stewart
Thank you for your letter. We are not prepared to reconsider your Correspondence submission. No doubt you will be able to publish your and your colleagues’ views on AIDS transmission in parts of Africa and elsewhere in the world in some other publication after peer-review, but Nature Correspondence is not an appropriate place for such reports.
Yours sincerely, Maxine Clarke, NATURE”
Here’s the text of the rejected letter:
(00 44) 0131 552 2648 29/8 Inverleith Place,
Gs2648@aol.com Edinburgh EH3 5QD, UK.
7th December, 2008.
resubmission, 15th December.
To: Dr Philip Campbell, Editor-in-Chief, NATURE,
By email to nature@nature.com Confirmatory copy in postal mail.
Response to THE COST OF SILENCE? Editorial. NATURE 2008; 456; 545.
The allegations and recent updates in your Editorial about avoidable deaths due to HIV/AIDS in South Africa certainly require attention, but need also to be corrected. In AIDS, of all diseases, silence is surely the wrong word. But noise, in local and increasingly in international medical journals and lay Media, was loud, resonant and viciously ad hominem in the year 2000 when ex-President Mbeki welcomed about fifty international experts to join what NATURE now refers to as “The infamous Presidential advisory panel”. I was invited in 1999 to join that panel in company with Professors Luc Montagnier, Peter Duesberg, Zena Stein, Etienne de Harven, scientists from the US NIH, physicians from the US CDC, the team from Perth (Australia) and experts from severely-affected locations in Africa, South America and elsewhere, and from main centres in South Africa. Dr Robert Gallo of the US NCI was invited to join but did not do so.
The infamous panel held meetings, at first in Pretoria and then in Johannesburg, chaired by a Canadian Judge, and taped. Observers from local and international Media were admitted to some meetings. Additional American experts, nominated by President Clinton, attended sessions and interviewed panelists individually and confidentially. The Minister of Health and the Chief Medical Adviser to the President attended all sessions, were available, with their staffs and other government officials and local academics, for consultation about transcripts and records, and to enable proposals made by members to be implemented, e.g. for ad hoc surveys and validation of tests. We were encouraged to visit clinics, laboratories, hospitals and, notably, old and new settlements at Soweto, Gauteng and MEDUNSA. To-and-fro activities on this basis continued through personal contacts and on the internet through 2006 when they were abruptly terminated by the sudden death of Professor Sam Mhlongo [footnote 1], who had been coordinating them. For this reason and because of fundamental and often sharp differences within the Panel, the outcome was, as Nature says, inconclusive, to which we would add a third word disappointing, because metropolitan facilities and expertise for investigation were impressive especially when in 2001 Dr Makgoba published a detailed report by the SA Medical Research Council. But their data and conclusions were found to be based [footnote 2] on records which were obsolete or incomplete. Do the recent reports to which Nature now refers correct this fault?
From 2000 onward, the noise increased internationally because seroprevalence of HIV and projections of symptomatic AIDS in Sub-Saharan Africa (SSA) were reported by UN AIDS, all major journals and health authorities as being the highest in the world (1-3). This was indubitable in continental comparisons but, within Africa, there were wide differences between the 50/51 countries where the data recorded in Sentinel Surveillance by WHO (2) showed a mean cumulative seroprevalence [footnote 3] of 126/100,000, higher than in any other continent or region. But this mean ranged from 39/100,000 (median 30) in 37, mainly northern countries, to a mean of 313/100,000 (median 268) in 16/50 countries in SSA, probably the highest in the world even with allowance for “Titanic” exaggerations and other errors, some of which were accepted as “Deliberate” by Nature (447;531-2) in their review in 2007 of disclosures (3) by James Chin, former Chief of AIDS for WHO before he retired to be a professor at UC Berkeley, CA. In South Africa, however, the mean was only 30/100,000. At all levels, these figures included doubts about incidence and projections based upon serotests, raised originally by Harvard field workers (4) in Africa and endorsed by Professor Mhlongo in SSA and in a communication to an open meeting on HIV/AIDS in Africa convened by and at the European Parliament in December, 2004.. However, as in other countries, and not only in Africa, validated data on sensitivity, specificity and consistency are still awaited. The massive registrations in tribal, borderline and backward regions are based largely on the infamous Bangui definition devised by WHO (5) for diagnosis of HIV/AIDS in places where there are no facilities for sampling, surveillance and testing, or even for recognizing and purifying dirty water.
High seroprevalence is not necessarily followed by increase in mortality or decline in population. In Uganda, formerly featured as the epicenter of the projected pandemic of HIV/AIDS, there was an unprecedented increase in population due to a slight decrease in mortality accompanied by a stable and higher birth rate over the period reviewed by the Infamous Panel (10).
These differences within Africa and between Africa and everywhere else require clarification as well as correction. When this was done in UK, USA and other developed countries, registration data from 1986 onward showed beyond reasonable doubt that the main determinants of symptomatic AIDS were and are high risk behaviours and preferences in sex, life styles and drugs (6-9), mainly in males, with transfer to female consorts bisexually and perinatally. In some other countries and especially in Africa, this transfer is complicated and extended (1,3,7,8) by abuse of women and girls in deeply unhygienic settings where all the STD’s and many other diseases (1,3,7-10) besides HIV/AIDS are endemic, often lethal and difficult or impossible to differentiate by the Bangui definition in the field or even in hospital, especially in infants.
Irrespectively of these desiderata, your editorial asserts that President Mbeki and his Minister of Health lost credit and support primarily because they had implied that HIV did not cause AIDS. Neither did Professor Montagnier in a paper (11) written with collaborators in 1990 and on other occasions ( before and since that important year).
REFERENCES
1 UN AIDS. International Registrations of HIV/AIDS. See also AIDS in Africa. EC Meeting, Brussels, Dec 8th, 2004; and Stewart, GT. AIDS and hepatitis Digest No 83; 2 (PHLS)
2 WHO: Sentinel Surveillance and wkly epidemiological reports. Geneva,1985-date
3 Chin J The AIDS Pandemic. Oxford, Radcliffe: 2007. See also Nature 200
4 Kashala O, Marlink H, Ilunga M et al. J Inf Dis. 1994; 169; 296,
5 The Bangui reclassification of AIDS. WHO, Geneva: 1985.
6 Stewart GT. Uncertainties about AIDS and HIV. Lancet 1989; 335; 1325.
7 Stewart GT Changing the case definition of AIDS. Lancet 1992: 340; 1414.
8 Bebe Loff Africans discuss ethics of biomedical research. Lancet 2002; 359; 956.
9 Stewart GT. Uncertainties about AIDS and HIV. Lancet 1989; 336; 1325
10 Uganda Bureau of Statistics 1995 and 2000-2001. Population Census 2002. …………..
11 Lemaitre M, Henin L, Montagnier L, Zerinal A et al. Res Virology 1990; 141; 5-16.
12 AIDS in Africa. The European Parliament, Brussels, December 2004.
13 See also Bauer HH The Origins, Persistence and Failings of HIV/AIDS Theory. Jefferson NC and London. McFarland Publishing: 2007.
14 De Harven E, Roussez JC. Ten Lies about AIDS. Victoria, BC., Canada. Trafford Publishing: 2008.
15 Other references and correspondence are profusely available, on request.
Footnotes:
1 See obituary, BMJ 2007.
2 See Fiala C et al Lancet 2001; 358; 1381 and correspondence with Department of Error.
3 Rounded to nearest whole number
Authors, with details for Editor:
Gordon Thallon Stewart, M.D., Emeritus Chair of Public Health at the University of Glasgow. Former consultant physician (Epidemiology and Preventive Medicine), NHS-UK., also to New York City, WHO, AMREF.; Emeritus Fellow, Inf Dis Soc of America and member, Editorial Board.
Etienne de Harven, M.D. Emeritus Professor of Pathology, University of Toronto. Formerly electron microscopist, The Rockefeller University, New York City.
Christian Fiala, M.D. Obstetrician-Gynaecologist in Vienna and Uganda.
Henry H Bauer, Ph.D. Dean Emeritus of Arts & Sciences, Professor Emeritus of Chemistry &
Science Studies, Virginia Polytechnic Institute & State University, Blacksburg, VA, USA.
Posted in experts, HIV skepticism, HIV/AIDS numbers, prejudice | Tagged: Christian Fiala, Etienne de Harven, Gordon Thallon Stewart, Jayne Henderson, Maxine Clarke, NATURE and censorship of non-mainstream views | 3 Comments »
PURIFY? WHO NEEDS THAT? (SO SAYS ROBERT GALLO)
Posted by Henry Bauer on 2008/01/17
It seems astonishing that hordes of virologists, immunologists, and other biological scientists should be wrong about HIV/AIDS. It is even more astonishing that HIV/AIDS researchers do experiments without caring whether the substances they are working with are pure.
Etienne de Harven, pioneer in the electron microscopy of viruses and Emeritus Professor of Pathology, University of Toronto, discussed in his address to the European Parliament [HIV HAS NEVER BEEN ISOLATED FROM AIDS PATIENTS, 15 January 2008] the failure of HIV/AIDS researchers to purify what they call “viral isolates of HIV”. Electron microscopy revealed that these “viral isolates” are motley mixtures of bits and pieces of various shapes and sizes; see “Cell membrane vesicles are a major contaminant of gradient-enriched human immunodeficiency virus type-1 preparations” (Gluschankof et al., Virology 230 [1997] 125–33); “Microvesicles are a source of contaminating cellular proteins found in purified HIV-1 preparations” (Bess et al., Virology 230 [1997] 134–44).
Phyllis Pease, emeritus in medical microbiology from the University of Birmingham, discusses in some detail the fact that “supposedly pure HIV as prepared by standard techniques for the isolation of retroviruses employed since 1970 [has been] without the benefit of essential electron microscopy controls” (p. 128, “AIDS, Cancer and Arthritis”, ISBN 0-9550567-0-5; see comprehensive review by Neville Hodgkinson at http://aras.ab.ca/index.php).
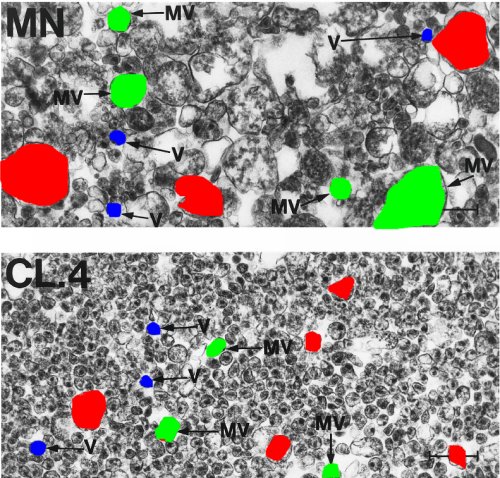
“Viral isolates” of “HIV” are whatever happens to be in the band of density 1.16, when a source thought to contain “HIV” is ultracentrifuged in a sugar gradient. Below is a tracing of electron micrographs published by Bess et al.; for easier identification, some of the microvesicles are colored green, some of the supposed virions are in blue, and some of the motley debris is in red. The lower micrograph is of a more highly purified preparation than the upper (see Pease, p. 129), yet still shows the presence of a variety of contaminants.
Not only are these mixtures of all sorts of things: when Pease measured the purported retrovirus particles (see p. 131 in her book), she found that their sizes spanned a wide range (70-225 nanometers). Purification had increased the proportion of virus-like particles, but clearly they are not all the same, as virions of a given species would be.
The astonishing, well-nigh incredible yet inescapable conclusion is this:
The “HIV” that researchers work with is a motley mixture of various kinds of intracellular particles (vesicles) and bits of cellular debris, in which there may or may not be present some particles of a putative human immunodeficiency retrovirus, and possibly other viruses as well.
This remarkable circumstance explains immediately several peculiar characteristics supposedly unique to HIV and that have made it so intractable a thing to deal with:
— No two HIV isolates are exactly the same. “Within a single HIV-1 infected human host, HIV-1 population represents a complex mixture, or swarm, of mutant virus variants, in which all viruses are genetically related yet virtually every virus is unique” (Lukashov et al., “The genetic diversity of HIV-1 and its implications for vaccine development” in AIDS Vaccine Research, ed. Wong-Staal & Gallo, chapter 3, at p. 93).
Of course! Every time researchers make a preparation of “HIV”, they are working with a different and possibly unique mixture.
— HIV is said to mutate at a rate far exceeding anything observed with other biological entities.
Not at all. Every time researchers make a preparation of “HIV”, they are working with a different and possibly unique mixture.
— Every attempt at preparing a vaccine against HIV has failed totally.
Naturally. One can’t vaccinate against motley mixtures of variable composition.
How do HIV researchers respond to the charge that their “viral isolates” are not pure HIV?
Whenever possible—which is most of the time—they simply ignore it, even since the cited articles, published in 1997. However, ignoring is not feasible if one is on the witness stand in a court of law, as Robert Gallo was (via telecommunication) at the Parenzee trial in South Australia. Here are extracts from the transcript of his testimony, which is available in full at http://garlan.org/Cases/Parenzee/:
“Once we could mass-produce this virus, that’s purification. If you have a tonne of something and you contaminate it by a drop of water, didn’t you purify it? It’s the ratio of cell protein to viral protein. Sucrose gradient gives you a little bit of help but you could do that five times and it’s not going to purify as much as we did by mass-producing it. To use the extreme hyperbole, if you have a tonne of some something and a drop of water, you’ve purified it. That’s what we did. (Emphasis added; p. 1278, lines 1–9):
. . .
We succeeded in putting six of the 48 isolates into permanent culture, meaning in a cell line, in a leukaemic cell line that, itself, doesn’t have virus particles, and the virus comes out in great quantity and forever, thus making purification already accomplished. But, of course, we also use banded virus by sucrose gradient which they make a case out of we never did. You don’t publish that. Of course we did, but it isn’t needed and wouldn’t be needed if you could mass-purify it. But, for other purposes, we did it. (Emphases added; p. 1278, lines 25–35).”
This is no inadvertent mis-statement, Gallo repeats it (Emphases added; pp. 1281, lines 21–37):
“people use great quantities of mass-produced virus which by itself is purified virus. You are not being told that either because they don’t understand it or they don’t know; I don’t know. It has gone through a far greater purification than any banding can produce. The blood test that became available to people who knew how to do it came from mass-produced virus, originally from in Frederick, Maryland. The genes now have been cloned. We started in publications in 1984 throughout 1985 which showed that each of the proteins you pick up with Western blot is coded by one of the genes of HIV or another. Therefore we know those proteins come from HIV and, when a patient’s serum reacts with them, we know that patient, untreated, will almost always get AIDS. You can’t get science any better or anything more definitive.”
***************************************************************************
Most scientists, I dare say most thinking people, would be astonished at Gallo’s assertion that if you have a large enough amount of something then it doesn’t matter what else is present. Perhaps he was aware of that when he made the disingenuous comment about “a drop of water” not being a contaminant, when the actual contaminants are an unholy mélange of things. Yet even a drop of water can ruin an experiment if that drop contains the tiniest bit of the wrong sort of substance.
Solid-state physicists had observed in the mid-1930s the phenomenon that led—but only 3 decades later—to the transistor revolution in electronics. During those 3 decades, the phenomenon could not be reproduced—because of the unknown and therefore uncontrollable presence of varying traces of impurities in amounts too small to be detected by then-available methods.
Much of my own work in electrochemistry had to do with a method known as polarography. Its discovery stemmed from a strange phenomenon whose very existence depended on the presence of impurities in amounts too small to be detected by any then-available means, something realized only some 5 decades (Bauer, “Streaming maxima in polarography”, Electroanalytical Chemistry, 8 [1975] 169-279). The sensitivity to impurities was so great in large part because polarography depends on reactions at surfaces. The tiniest amounts of impurities in a solution may accumulate at surfaces to produce tangible effects. Many processes that depend on catalysis are surface reactions. The ubiquitous enzyme reactions in biological systems are essentially catalytic surface phenomena: the reacting substance has to fit precisely onto the surface of the enzyme. Contaminants in biological systems can ruin experiments and vitiate entirely any claimed results.
It beggars belief that a scientist would ignore the relevance of possible impurities in biological research or attempt to down-play the possible significance of impurities.
Posted in HIV absurdities, HIV tests | Tagged: electron microscopy of HIV, Etienne de Harven, HIV electron micrographs, HIV isolation, HIV pictures, Phyllis Pease, pure HIV, purifying HIV, Robert Gallo, viral isolates | 24 Comments »
